
What Is A Brachial Plexus Injury?

Raynes Lawn Hehmeyer, a national practice representing families with babies who have suffered spinal cord injury, brachial plexus injury, Erb’s palsy, and Klumpke’s palsy
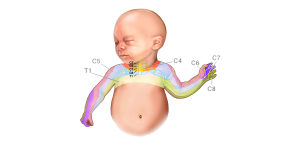
The brachial plexus is a crucial bundle of nerves that exits from the lower cervical and upper thoracic portions of the spinal cord and controls function in the shoulder, arm, and hand.
When an obstetrician or midwife delivers a baby, the infant’s shoulder can get stuck behind the mother’s pubic bone. This is called “shoulder dystocia.” In this situation, the practitioner delivering the baby must take great care not to pull or twist the baby’s head.
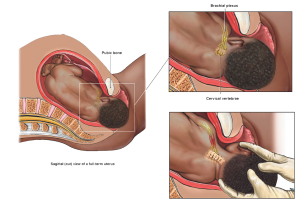
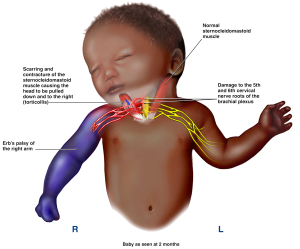
Forceful pulling or twisting may damage these nerves permanently, impairing function and, in the worst cases, making the arm unusable forever.
There are a series of proven maneuvers to relieve a dystocia and release the shoulder without putting risky traction on the baby’s head and neck. First, the nursing staff must bring the mother’s knees back as far was possible in what is called “McRobert’s position.” (As shown below #1) Next someone on the delivery team applies “suprapubic pressure” by making a fist, placing it just above the maternal pubic bone, and pushing the fetal shoulder in one direction or the other. (As shown below #2)

geraldbaeck [CC0], via Wikimedia Commons
If that is not successful delivering the baby’s stuck shoulder, the doctor or midwife then reaches inside the mother’s vagina and pulls out the baby’s “posterior arm,” meaning the arm on the side that is not stuck on the pubic bone.
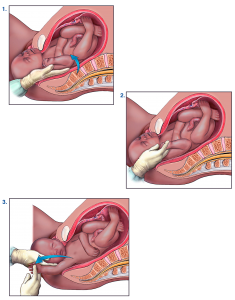
Finally, the baby is rotated so the impacted shoulder comes off the pubic bone – at which point the baby should deliver without permanent injury.
There are certain factors that place your baby at a higher risk for shoulder dystocia, such as large infant size, gestational diabetes, high birth weight, above normal weight gain during pregnancy, breech position and small maternal size. It is your doctor’s job to account for these potential risk factors and recommend a cesarean section to avoid complications if they pose significant risk. In some cases, failure to recommend a cesarean section is malpractice.
There is a disturbing trend among obstetrical/family practice training programs to allow residents (medical trainees) to attempt to deliver a baby when there is a true dystocia with too little or even no training. This can cause a catastrophe. The current medical standard of care requires doctors in training and even experienced doctors to undergo regular dystocia simulation training. Here is a link to an example of a shoulder dystocia training simulation:
In our experience, virtually all spinal cord injuries and permanent brachial plexus injuries, evident shortly after birth, are medically preventable and result from medical malpractice – either the failure to recommend a cesarean section, inadequate or improper training, or pulling/twisting the baby’s head too hard.
If your baby has been injured, we can pursue compensation for the significant medical expenses associated with your child’s surgical and non-surgical treatment and therapy. We also can seek compensation for the pain and suffering you and your child endure and your child’s reduced earning capacity and quality of life due to the injury.
Our attorneys frequently represent clients whose child has suffered a brachial plexus injury. For more information about our experience with shoulder dystocia, brachial plexus injuries, Erb’s palsy, Klumpke’s palsy, spinal cord injuries and related birth injury claims, contact the national brachial plexus injury attorneys at Raynes Lawn Hehmeyer at (800) 535-1797 or (215) 568-6190 to schedule a free case review.